Sciatic pain — the deep, radiating discomfort that travels from the low back into the buttock and down one or both legs — is a symptom most of us associate with disc problems, spinal stenosis, or muscle tightness. But for many people who struggle with chronic or recurring sciatica, conventional explanations don’t fully account for why the pain persists or shifts over time.
In the work of French osteopath and physical therapist Jean-Pierre Barral, sciatic pain is understood not just as a mechanical problem of the spine, but as a symptom that can arise from deeper organ, fascia, and nerve restrictions throughout the body. Two branches of his manual therapy — Visceral Manipulation and Neural Manipulation — explore how restrictions in organs and nerves can create tension patterns that ultimately contribute to sciatica.
In this article, I’ll explore five causes of sciatic pain from an integrative perspective so patients can better understand possible contributors beyond the spine itself.
1. Organ-Related Tension Patterns (Visceral Restrictions)
One of the foundational ideas in Barral’s approach is that the internal organs (viscera) are not static — they move with breathing, posture, and everyday activity. Visceral Manipulation helps restore this natural mobility and examines how restrictions in organ motion can produce abnormal tension throughout the body’s connective tissue (fascia).
How This Relates to Sciatic Pain
Your organs sit within a network of ligaments and fascia that attach to the spine and pelvis. If an organ develops adhesions, restrictions, or abnormal tone — through surgery, trauma, inflammation, poor posture, or even digestive disturbances — those forces can create tension that radiates outwards. This can change how muscles and fascia around the hip, pelvis, and lumbar spine function, and can indirectly influence the sciatic nerve’s environment.
For example, tight fascia or connective tissue adhesions around the ascending colon or right kidney might contribute to right-sided sciatic pain by influencing the way these structures connect tension patterns across the low back and pelvis. Similarly, tension in the sigmoid colon (the lower left part of the large intestine) can be associated with left-sided sciatic pain because of its connective tissue relationships with pelvic and lumbar structures.
These connections are not obvious in conventional anatomy charts, but in Barral’s clinical experience, the body responds as a whole, integrated system, not as isolated parts.
What Patients Often Experience
People with this type of visceral influence on sciatica may notice pain that doesn’t follow a typical dermatomal pattern (i.e., exactly where nerve roots exit the spine), sciatic discomfort that comes and goes depending on digestion, constipation, or abdominal bloating, and pain that shifts from one side to the other over weeks or months without a clear mechanical trigger.
This doesn’t mean the cause is in the abdomen — but that fascial and organ restrictions can contribute to tension patterns affecting the sciatic nerve’s pathway.
2. Nerve Fixations and Restricted Neural Mobility
Another key branch of Barral’s work is Neural Manipulation, which focuses on the nerve itself — not just where it exits the spine, but how it glides and moves through surrounding tissues such as fascia, muscles, and narrow tunnels.
Understanding Nerve Movement
Nerves are designed to slide, stretch, and adapt as the body moves. This “neural glide” is essential for healthy nerve function. When nerves become fixated or lose mobility — often due to adhesions in connective tissue, scar tissue from injury or surgery, or prolonged postural strain — they can become hypersensitive.
A nerve that can’t glide freely may become compressed under surrounding structures, experience changes in blood supply, “stick” at certain points in its length, or develop tender connective tissue nodules (“nerve buds”) that indicate areas of fixation. All of these factors can disturb how the nerve conducts signals and contribute to pain that patients interpret as sciatica.
Below is a video of a neural manipulation treatment as performed by Chris Gauntlett in clinic.
How This Leads to Sciatica
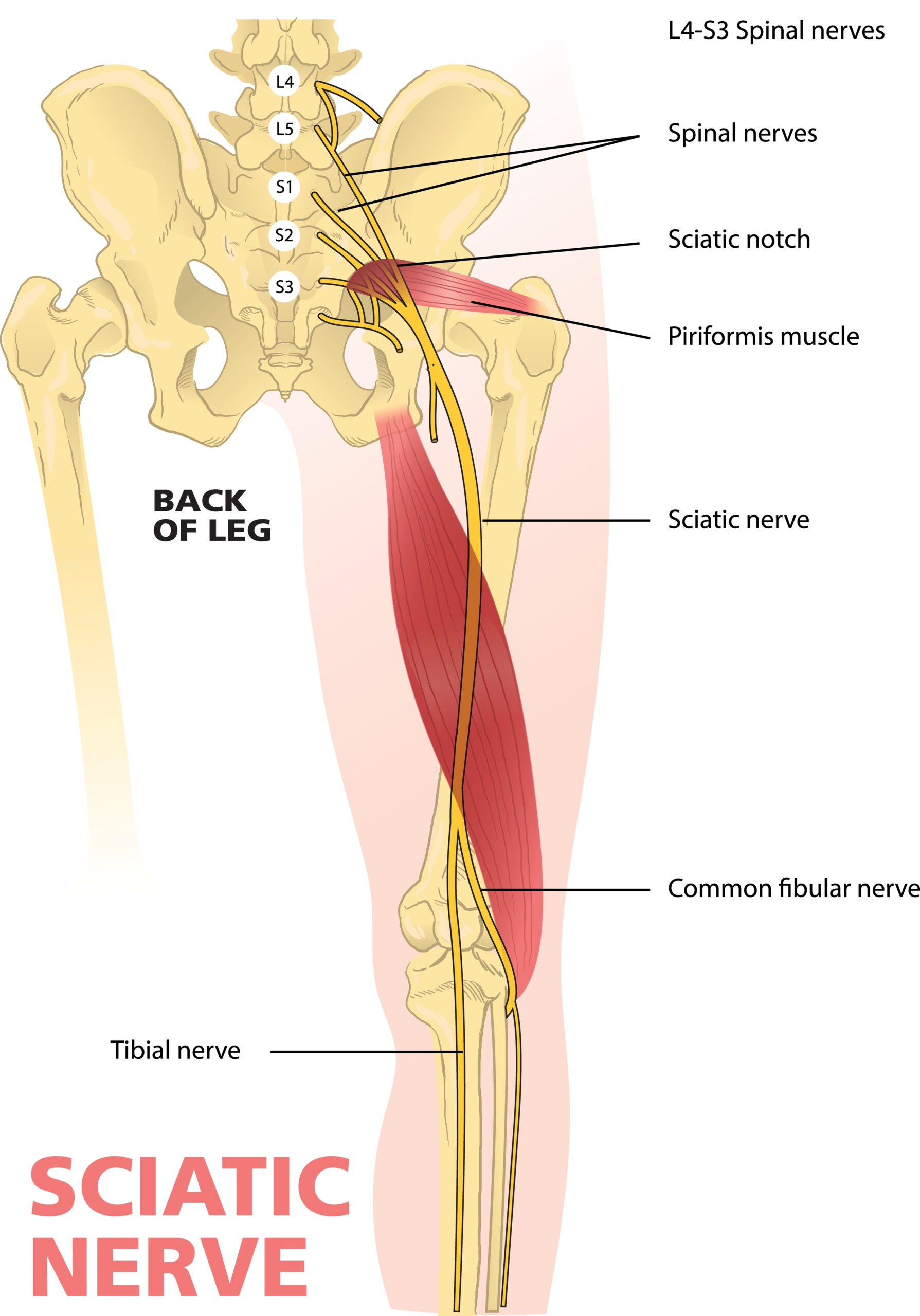
The sciatic nerve is the longest nerve in the body, extending from the lumbar spine through the pelvis and down the back of the leg. It passes under or through several muscles — including the piriformis — and through fascial layers that can become dense or restricted.
If the sciatic nerve is compressed by tight muscles or fascial restrictions, restricted by scar tissue, or unable to glide during movement, it can signal pain that mimics classic sciatica, even if the spinal discs themselves are not severely damaged.
What Patients May Feel
Patients may experience burning, tingling, or shooting pain that isn’t fully explained by spinal imaging, pain that worsens with specific movements where nerve glide should occur (like bending forward or side-to-side rotation), and tender spots along the nerve path that feel sensitive to manual touch.
3. Fascial and Pelvic Ligament Imbalance
Barral’s approach also acknowledges that fascia — the connective tissue web that envelops muscles, organs, nerves, and bones — plays a major role in how forces are distributed across the body.
Fascial Tension and Sciatica
Fascia can become restricted through scar tissue from past injuries or surgeries, postural stresses (e.g., sitting for long periods), repetitive strain, and inflammation from digestive or visceral disorders. When fascia around the pelvis or lower back becomes restricted, this can alter the alignment and movement of the sacroiliac joints, hip joints, and the muscles surrounding the sciatic nerve. The fascia can essentially “pull” the structures out of their optimal motion patterns, creating compressive or traction forces on the nerve.
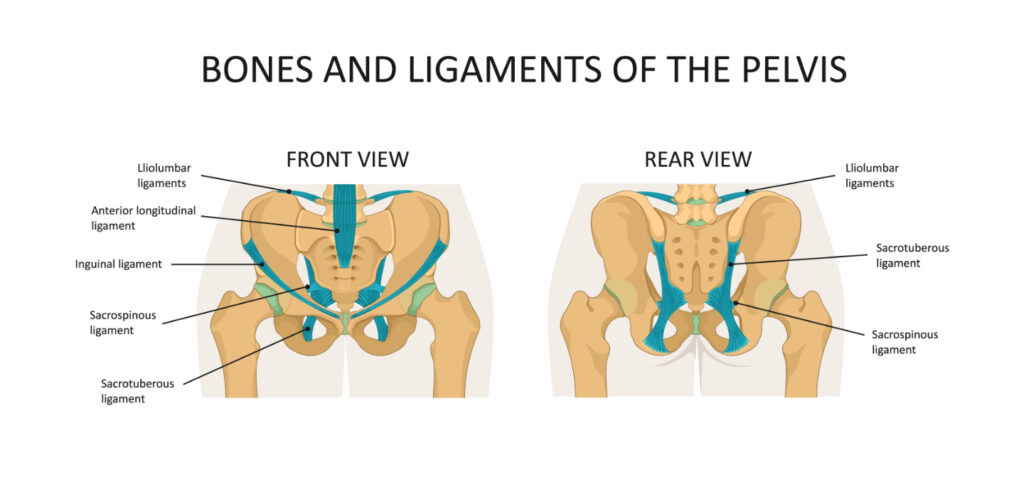
Two examples of ligaments that are often witnesses to intrapelvic torsion and sacroiliac dysfunction are the sacrotuberous ligament and sacrospinous ligament. These ligaments are areas commonly requiring treatment in clinic.
Pelvic Ligaments and Organ Suspension
Internal organs are held in place by ligaments that attach to the pelvic bones and low back. If an organ’s mobility is lost, its ligamentous connections can transmit tension into the pelvic girdle — potentially affecting the piriformis muscle, sacrum, and surrounding fascia. This is a common theme in Barral’s work: organ restrictions influence musculoskeletal mechanics.
Symptoms You Might Notice
Patients may experience pain that feels deeper in the pelvis or buttocks rather than just along the sciatic track, uneven pelvic motion during activities like walking or climbing stairs, and a sense that one leg or hip feels “different” than the other, even without obvious muscle weakness.
4. Dural Tension and Whole-Body Nervous System Effects
While less commonly discussed in mainstream therapies, Barral’s work also considers the role of the dura — the protective membrane surrounding the brain and spinal cord — and its mechanical relationship with nerves throughout the body. This is part of Neural Manipulation training.
Why Dural Tension Matters
The dura doesn’t just encapsulate the spinal cord; it extends down through the vertebral canal and merges with nerve roots. Tension or fixation in the dura can create a global tension pattern that affects how the spinal nerves (including those forming the sciatic nerve) glide and respond. Because the nervous system is continuous, restrictions high up — even near the cranium — can influence tension lower down. In Barral’s teaching, this is part of understanding how cross-talk and global neural dynamics can emerge.
How This Can Present
Patients with dural tension patterns may experience sciatic-like symptoms that don’t correlate with a specific spinal level injury, sensitivity in multiple body regions, and a sensation of “tightness” in the nervous system that does not resolve with typical muscle stretching. This is closely related to the idea that, when restricted, the nervous system can send excessive signals to muscles and fascia, contributing to pain and dysfunction.
5. Visceral Vascular and Circulatory Influences
A less-obvious yet insightful concept in Barral’s broader manual therapy repertoire is Visceral Vascular Manipulation, which focuses on the fluid dynamics around organs and their blood supply. While not directly the first line for sciatic pain, circulatory influences can contribute to the environment of the nerve.
Why Blood and Fluid Matter
When blood flow or lymphatic drainage is compromised around an organ, it can increase local inflammation, create swelling that pulls on fascial structures, and alter how tissues around nerves and joints respond to movement. Because the fascia around organs continues into the pelvis and lower back, circulatory disturbances can create secondary tension patterns that interact with sciatic nerve pathways.
For example, venous congestion in the lower abdomen can create tension that travels into the pelvic connective tissues, affecting the nerve sheath around the sciatic nerve. This may be more noticeable in people with digestive symptoms, pelvic congestion, or lower limb heaviness.
Bringing It All Together: What This Means for You
Jean-Pierre Barral’s perspective challenges the idea that all sciatic pain is purely mechanical (e.g., disc herniation pressing on a nerve root). Instead, it invites us to see the body as a connected, dynamic system, where organs communicate with muscles and fascia through connective tissues, nerves need freedom to glide and adapt, and restrictions anywhere in this system can influence pain patterns elsewhere.
Visceral and Neural Manipulation don’t replace traditional medical evaluation — especially if symptoms are severe, progressive, or accompanied by neurological deficits — but they may offer insight into cases where pain doesn’t respond fully to standard treatments, diagnostic imaging isn’t conclusive, or symptoms fluctuate with digestion, posture, or movement.
If You’re Considering This Approach
Ensure a thorough examination by a qualified practitioner who understands both conventional and manual therapies. Ask how visceral and neural assessments are performed — experienced therapists use gentle palpation and movement testing. Understand that these therapies are generally gentle and precise, aiming to assist natural motion rather than force changes. Discuss any digestive, pelvic, or systemic symptoms you may have, as these can be relevant in an integrated model.
Final Thoughts
Sciatic pain is complex, and no single explanation fits everyone. By appreciating how the organs, nerves, fascia, and connective tissues interact, you can open new avenues for understanding and managing your pain. Whether through Visceral Manipulation, Neural Manipulation, or traditional therapy, the goal is the same: to restore harmony, reduce tension, and improve function — from the deep inside out.




